



Covid Shots Cause Immunodeficiency
New Yale study finally proves what we've known for years.

Since 2020, long before the shots were even available, I have been warning that the spike-based vaccines would cause immunodeficiency. Given the fact that the virus itself had been engineered to include HIV proteins on the spike, it was all but a foregone conclusion. Of course, between the din of the progressive propaganda networks treating any criticism of them as heresy, and the lunatics and controlled opposition trying to tell you that viruses themselves don’t even exist, the truth has long been waiting for its day in the light.
Well, the science has caught up, and now that truth is finally coming out in a form that cannot be denied any longer. Specifically, progressively mounting deficiencies in CD4 T-cell counts have now been measured - alongside the persistence of spike proteins in the blood, now detected, in a new record, up to 709 days post-vaccination - in 66% of the Covid vaccinees studied here.
In light of this, the administration is - despite the attacks from a few of the people that found themselves, to their surprise and indignation, not to be part of it - now moving quickly to completely halt their availability. There’s a certain bittersweet quality to watching some of that drama; it cost me dearly, but I couldn’t be happier with some of the people that are, and are not, calling the shots now. It’s something of an open secret that just about everybody around him these days knows exactly what’s up with the shots - but when your entire public personality has been built around narrative self-promotion, some doors are closed for good. Some chose popularity. Some chose to get it done right. You’ll never hear from most of the latter.
I’ll tell you a secret - now that a little time has passed - Trump likes vaccines! Shocking, I know. The straight up anti-all-vaccines position is a crowd pleaser, it’ll get you the likes and the follows, the fame and the fortune and the Swiss mountain retreats - but it’s not going to get you anywhere under a President that remains to this day very proud of having brought those vaccines to market at “warp speed,” even as the signs mount that maybe it wasn’t such a good idea. There will be accountability, and there will be justice, but it won’t be wrought by the glory hounds that care more for the fame and the accolades than they do for the fight. There also remains extremely broad support for vaccines in general, among older people and that silent majority that never spent enough time on social media to see what’s been happening; if that fight is to be won, it will be won by the hard science that can be understood by all, being presented by unimpeachably neutral scientists. It will take time, and it will take credibility, and RFK’s brilliant strategy - “vaccines are great actually, let’s just make sure they’re safe (they’re not)” - is absolutely incompatible with having pigeonholed oneself into complete inflexibility. I know they’re not, and you know they’re not; they tried to derail his nomination by calling him an anti-vaxxer, and seeing as he’s very well maintained that he’s not, they failed. With that degree of political acumen heading up HHS, we have a once-in-a-generation chance, and there’s no room for the showboaters.
But, for now - let’s dig into exactly what’s just been “discovered” here, five years of warnings and dismissals, and over a year after the study itself was concluded, later.
The Study
The cross‐sectional case–control study was conducted between December 2022 and November 2023 under the Yale LISTEN framework. 42 individuals reporting chronic post‐vaccination symptoms, and 22 otherwise healthy vaccinated “controls,” were enrolled. Notably, the “healthy” control group had a median of only 199 days since their last shot, whereas the injured group had been vaccinated around 585 days earlier. Even just on that, we can draw a conclusion: the more time that passes, the more damage is done. As we’ve already learned, quite some time ago, the production of spike protein does not cease, and we now have a new record of continuous production up to 709 days post-vaccination; it probably declines as infected cells are destroyed over time, but it’s not going anywhere anytime soon. They’ve turned billions of their cells into semi-permanent factories that ceaselessly produce billions of microscopic needles for years afterward; now the results are finally being quantified.
As for the specifics: the injured group had reduced levels of both memory and effector CD4 T-cells, significantly below the expected range; significantly increased TNFα-positive CD8 T-cells, indicating an elevated inflammatory response; lower anti-spike antibody levels, relative to controls; and elevated levels of free, circulating spike protein.
Interestingly, what isn’t present is the actual blood counts. The study presents them only as percentages of what would be normally expected (generally in the ~42% range). Depending on the baseline, which isn’t given, ordinary minimum T-cell counts are around 500 ng/ml; any lower than that and you’re squarely into AIDS territory. 42% less than that? Putting those raw numbers in the data would be a blazing signpost declaring that they’ve all got, or will have, AIDS. It still is, but it’s not presented quite so plainly for a lay reader. Probably would’ve been tough to pass peer review if they made it that clear.
There’s a lot more ancillary data if you care to review it, but the upshot is that their immune systems have been decimated, they’re not responding as strongly to the spike anymore - which is still present, circulating in the blood and doing damage, years after vaccination, despite all those promises that it would be gone after a few days - and they’re suffering chronic, debilitating inflammation.
How It Actually Happened
So, we know that the vaccines are causing a slow-burn immunodeficiency. A person takes the vaccine, takes a booster or two or five, and months to years later, a substantial proportion of them find themselves with a brand new immunodeficiency. That much has now been proven in black and white. The question remains: why?
It all starts with a protein called gp-120. This is a protein on the spike of the HIV virus: it enables HIV, alongside CCR5, to interface with the CD4 and CCRX4 receptors on CD4, to infect and begin replicating inside of CD4 immune cells. As I covered in my broad exploration of the immunology here, CD4 are the colonels of the immune system’s army; they send and receive chemical signals, from infected cells, from foreign infections, and from other elements of the immune system, and activate the various localized immune responses. One of the hallmarks of HIV is a steadily declining CD4 count and the virus being detectable inside the cells that are supposed to be guarding against it.
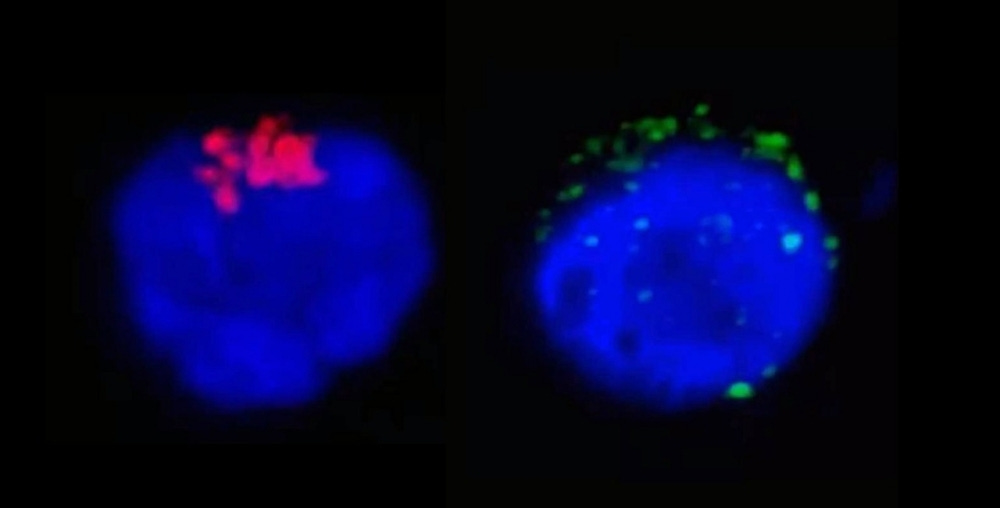
One of the very first revelations, extremely early in the pandemic, and quickly shut down by Fauci, Birx and Collins’ machinations to discredit and suppress any scientific findings that contradicted their various fairy tales, was that the gp-120 protein had been engineered into the SARS-CoV-2 virus. Interestingly, it was missing the other half of what’s usually necessary for HIV to infect a CD4 cell; the gp-41 protein, which interfaces with the CCR5 receptor and permits a viral infection of the cell, was not included alongside gp-120. The upshot of that is that, rather than infecting the cell - usually, anyhow - the spike protein would simply set off alarm bells in the CD4 cell and cause it to self-immolate. With the activation of that secondary receptor, the cell continues to believe that all is well; without that interaction, it becomes aware that it is under attack, and usually self-destructs. It’s not 100%; some SARS-CoV-2 infections of CD4, just as occurs in HIV/AIDS, have also been detected and imaged.
SARS-CoV-2, and most enveloped viruses, bud out from the surface of the cell, binding and encapsulating the spikes and ssRNA in the process, and taking a little bit of the lipid cell wall with it. This method enables it to reproduce and spread rapidly, without directly killing the cells it occupies. This enables, under the right (wrong) circumstances, a far more persistent infection, as it does not need to destroy every cell it infects in order to spread.
As I’m sure you’re aware, the SARS-CoV-2 virion is coated in spikes. They’re the mechanism by which it interacts with ACE-2 and other receptors to propagate its infection of the various cells it’s able to enter. A single virion is tiny; 1000x smaller than a CD4 cell, with dozens of those spikes affixed to its surface. When a single virion interacts with a cell, only one of its spikes is engaged and binds to the receptors; the rest of them, presuming a successful infection occurs, are subsumed into the cell along with the first one, and destroyed by proteases and lysosomes inside the cell. Every engineered gain-of-function addition to the spike is present in both the virus and the vaccine, and thusly, have the same effects, regardless of the form - with the curious exception of every strain from Omicron forward, which lost the most severe of the gain of function insertions, to Bill Gates’ dismay.
The major difference between the mRNA shots, versus the virus, is that there are trillions of free spikes floating around. With a single virion, you’ve got dozens of spikes, only one of which will ever interact with anything of relevance. When you turn a billion cells into spike factories, and they eventually fill up, burst and die, and release their spikes, every single one of them is capable of destroying anything it touches. It binds to red blood cells and platelets, which can cause the proteinaceous “clots” that have frequently been observed in the victims who have later died from them; and they cause extensive inflammatory damage to the epithelial linings of blood vessels large and small, which doesn’t help - picture a wall in a warzone, pockmarked with bullets and shrapnel, and that’s your blood vessels - and they can single-handedly cause abject chaos and destruction as they encounter and destroy CD4 T-cells.

It has also been proven, several times now, that everything else they said about how the mRNA vaccines work was not true: they do not stay in the arm, they do not quickly - or perhaps at all - cease spike production, and even the lipid nanoparticles themselves are devastating to reproductive function, amongst other things.
A Permanent, Slow-Burn Immunodeficiency
So, let’s connect these dots.
LNP-mRNA shots create continuous, long-term production of free, soluble spike proteins, that permeate the entire body.
Those soluble spike proteins contain the same HIV epitope, gp-120, that was engineered into the original SARS-CoV-2 virus;
Those soluble spike proteins are thousands of times more dangerous than those attached to the virus itself, simply because they are orders of magnitude more biologically active, not being confined and attached to any one virion.
Long-term CD4 deficiency has now been conclusively characterized and proven in vaccine recipients, and not found in unvaccinated or Covid-infected patients.
What does it mean?
They gave you AIDS. Acquired Immunodeficiency Syndrome. They have acquired, from the vaccine, a syndrome, among the symptoms of which is immunodeficiency.
Some of us tried to warn you.

So, what can I do?
Well, this is where it gets interesting. Typical HIV medications, anti-retrovirals, work by suppressing the replication and proliferation of the HIV virus itself. That’s really not an option in this case: there is no replicating virus, there is only pseudouridinized mRNA, designed for long-term persistence to resist breakdown by natural cellular mechanisms, engaging with the regular cellular machinery that produces all the other proteins that are critical to life as we know it. There is no “off” button for the ribosomes, and if there were, you would die a very quick death, not unlike radiation poisoning, if you used it.
You don’t have HIV. You have AIDS. The distinction is very important. An interesting note here is that the tests that are generally in use do not detect the HIV virus itself; some more recent tests check for antibodies, but generally, they check the blood volume counts of CD4 T-cells, and an immune count below the critical threshold of 500ng/l is a positive result for AIDS; the lower the count, the more advanced the disease, and the more apparent the symptoms of a slowly failing immune system.

While there is no single cure yet - in light of these revelations, this will have to become a high priority for the newly reformed agencies under RFK and HHS - there are several promising approaches, some of which can be used now, some of which will require extensive further research and development.
1. Attack The “Infected” Cells
The “vaccine” works by inserting lipid nanoparticles, or LNPs, into the tissues and bloodstream; much like releasing a soap bubble into a crowd of other soap bubbles, most of the cells in our body also have lipid surface layers, and when the particles encounter a cell, their surfaces merge, enabling the LNP bubble to deposit its mRNA contents into the cell. That mRNA is then processed by the ribosomes, which produce the spike proteins. They then float around the cell, occasionally attacking some of the cell’s natural defense mechanisms against cancer; some migrate to the surface, where they penetrate and present on the surface. That presents an opportunity.