

New Study Confirms IgG4 Class Switch
mRNA vaccines increase susceptibility to severe disease.

The bad news just keeps coming for the mRNA guinea pigs.
I wrote, a couple of years ago, about the likelihood of mRNA vaccines inducing an IgG4 class switch, and the consequences that would have for those who took those shots. In short, because of the long-term persistence of the spike protein, instead of staying in the arm and being gone in a couple of days as was promised, that persistent exposure, lasting months, years or potentially indefinitely, instead trains the immune system to ignore and disregard a viral infection. Similarly to the archetypal case of pollens, when an otherwise healthy immune system encounters a foreign body, and it persists for long enough, the body undergoes a cascading response, switching between IgG subclasses from one, to two, to three, and eventually arriving at IgG4.
IgG4 is called the anti-antibody. Every antibody subclass serves as a flag for the immune system. With classes one through three, and from the broader IgM/IgA types that will bind to nearly anything, versus the custom-made IgG type that is produced to bind to one specific antigen, one recognizable part of some foreign body, the antibody activates the rest of the immune response; the complement cascade begins, various immune cells release signaling chemokines and cytokines to recruit immune cells to the site of the infection, and the immune response begins in earnest. In contrast, IgG4 serves the opposite purpose; the immune cells that meet it will be disabled, the local complement cascade will be interrupted and pacified, and the immune system is told, “Don’t worry about this one. He’s harmless.”
This is a necessary adaptation to prevent an otherwise damaging inflammatory response to ever-present foreign bodies such as pervasive pollen in the spring. The failure of this mechanism, among others, manifests as hayfever; a completely pointless, damaging inflammatory response is induced, where none is necessary. A few molecules of pollen (generally) aren’t actually going to hurt you; IgG4 is among the body’s mechanisms to recognize that, and call off the cavalry.
What you don’t want is an IgG4 response to a replicating pathogen that is going to harm you - and that’s exactly what the mRNA shots are, quite foreseeably, causing.

A new, preprint study, just published from the University of Amsterdam, has confirmed exactly what we said was going to happen: after a long delay, up to six months or more after taking at least two shots, the immune response in mRNA vaccinees eventually switches to the non-inflammatory IgG4 subclass.
This is bad news bears for, it appears, anybody that took those shots.
The Study
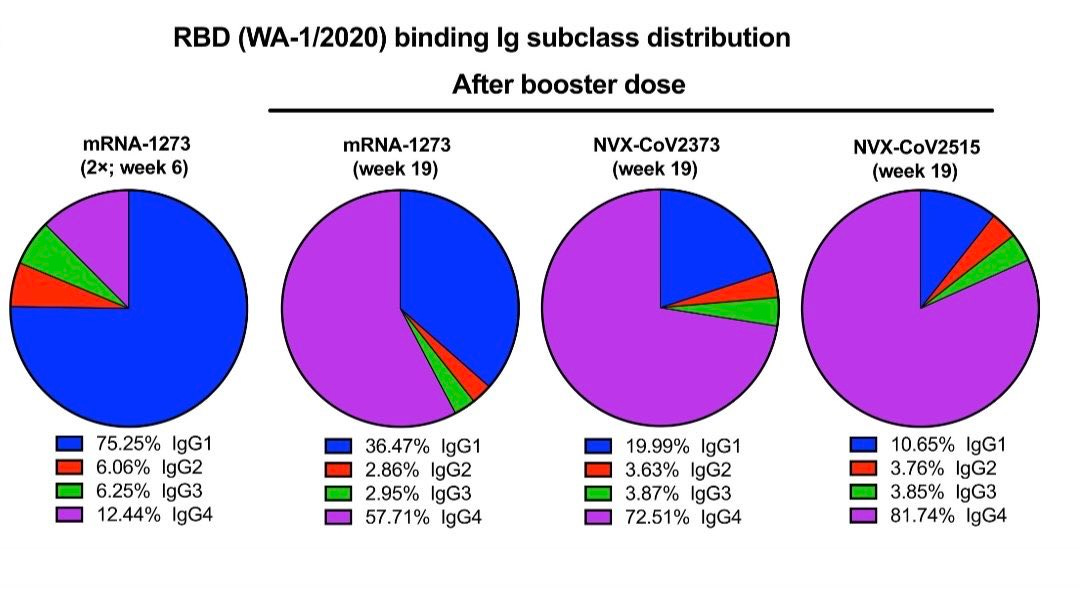
The researchers followed four cohorts of patients undergoing treatment for kidney disease. The study included only those who had taken at least two COVID-19 mRNA “vaccines,” and studied the patients’ immunologically healthy, unvaccinated family members or close associates for their control groups. Baseline levels were measured 28 days after vaccination, with IgG4 consisting of 3-5%, versus IgG1 at 55-65%; later, between two and six months after their second dose, almost all of the studied patients had substantially elevated anti-Spike IgG4 levels, up to five times their starting prevalence at 10-15%, with subtypes two and three having all but vanished, and IgG1 levels remaining stable.
This is an interesting development. In a full class switch, IgG1 tends to vanish almost completely, to be replaced with IgG4 almost exclusively. Here, only IgG2 and IgG3 vanished, and IgG4, rather than completely taking over, was only elevated in the response, with IgG1 proportions remaining stable.
The effect documented in this particular study is in fact substantially milder than some previous studies. A favored strategy for bad science is to publish the data, and then to mess with the abstract and conclusions - for a generation of practitioners who slept through school, unable or unwilling to actually read beyond the headlines, it’s a very simple matter for one’s conclusions to bear absolutely no resemblance to the data they’re drawn from. An earlier study, this one in 2023 (h/t Dr. Lynn Fynn for bringing it up, thank you!), showed a post-vaccine IgG4 dominance up to 80% in animal studies - and still managed to endorse them in the abstract. That alone should have been enough to hit pause on this. Thank God that our immune systems are a little more resilient than those of our primate cousins.
Complete vs Partial Class Switch
The subtlety of the switch belies its effect. IgG4 is a potent immunosuppressant; it does not need to completely take over to exert an outsized effect. Most of the body’s systems rely on homeostasis, and various levels of signal and countersignal, as I’ve covered in previous articles; a given pathway will be affected by both agonists and antagonists, with competing levels of “peace” versus “war” signals, and the eventual response will be determined by which is stronger at any given time.
IgG4 works a little differently. When an immune cell responds to an IgG1 antibody, it’s likely only there because it’s already been summoned to the site of infection; some cells will continue to amplify the signal, while most will just get to work attacking the foreign body. An IgG4 response, on the other hand, takes priority. The antibody manually interrupts the complement cascade, binding to C3a, preventing C3b deposition; immune cells that are told to stand down will reliably repeat and amplify those orders. One IgG4 calling for peace will be heard and amplified more loudly than ten IgG 1-3 encounters.
Of course, there is a silver lining. The fact that IgG1 remains dominant means that, at any given site of infection, there’s a reasonable chance that there won’t be any IgG4 present for at least a while, and the immune system will still be able to do most of its work. If IgG4 were dominant, the effect would be comparable to AIDS; even with an otherwise healthy immune system, even boosted in its power by the common C and D vitamins, the response would be completely shut off, and the viral infection would be free to run rampant, causing extensive tissue destruction, blood clotting, releases of stressor chemokines, and the various other unavoidable signals induced by cell death, until it ends up overwhelmed by that pervasive counter-signal; at that point, very late in the course of an infection run rampant, a cytokine storm would commence, with the body realizing it has some catching up to do against that infection; inflammatory artillery starts firing everywhere, all at once, and massive tissue destruction and death follows in relatively short order without intensive medical care, and even then it’s a crapshoot. Cytokine storms were, for a time, the leading, direct end-stage cause of death for those in hospital with severe COVID-19, frequently following bacterial infection from incompetently executed intubations causing mechanical injury to throat or lung tissue.
The Immune Microenvironment
An immune response is, generally - except in cases of cytokine storm - hyper-localized to the site of infection. Consider that everything that constitutes the immune system is carried in and by the blood, which is constantly rushing by, never static. Immune cells that were, five seconds ago, moving through your heart, calmed and idled by the absence of any antibody or chemokine signal, only momentarily find themselves, by pure chance, rushing by the site of an infection and suddenly in receipt of that alarm.
The alarm, too, travels through the blood. A cell that releases an alarm, in the form of various molecular chemokines or cytokines, will see those molecules rushed away in the bloodstream. Immune cell motility - their ability to choose a direction in which to move, to follow an alarm to its source - is based upon these cytokines. A CD8 cell in your leg, where nothing in particular is going on, will be in an environment that is saturating it with ‘peace’ signals; when it smells an alarm, it will physically move in the direction of that alarm, trying to get closer to the site of infection.
As it moves closer to the site of infection, that signal gradient will gradually shift away from the bias toward peace, and the volume of that alarm will steadily increase; closer to the infection, there are more cells releasing those alarms, and increasingly fewer ‘peace’ signals. This balance is instructive to the cell as to whether it needs to be in attack mode yet.

IgG4 is among the strongest ‘peace’ signals. As it processes the increasingly pervasive gradient of alarm signals, and draws closer to the site of infection, it’s still being saturated with both types of general signals; if it started in the leg, and an infection is in, say, the groin, the cells in the knee are still saying everything’s fine, but that smell of danger is getting stronger. The most effective cells aren’t generalists; CD8, the heavy artillery, are largely produced specifically to respond to one epitope of one hostile foreign body. While the immune system is ever present, we don’t walk around with an army of cells ready to attack some specific pathogen or another. There’s billions of potential pathogens, with billions of potential protein conformations that could be recognized by any one cell; we can’t keep them all, in quantity, all the time. While there’s generally some present, for most types of potential infection, their quantity is minimal and residual from the last time that pathogen was seen in the body.
That is also, coincidentally, the reason why the practice of measuring actively circulating antibody levels against SARS-CoV-2, as a proxy for whether one is protected, or in need of another booster, is quite insane. That faulty approach was used to justify instructing people to get one booster after another: just one more of the genocidal frauds perpetrated on the world by Dr. Fauci.
A properly established immune response will create memory B-cells, which then sit idle until their pathogen is encountered, and only then will they flood the body with antibodies and immune cells tailored to that pathogen; it is not natural to walk around with persistently high levels of antibodies for a pathogen you have not recently encountered. That is the primary reason this class shift has occurred - that unnatural, ever-present exposure is what drives the class switch. The logic that evolved here is, effectively, that if we’ve been on consistent high alert against a foreign body, that has been continually present for six months now, and you’re still here to tell the tale, then it’s probably harmless, and your immune system should stop overreacting.
This is also a major method by which immunological cancer therapies will eventually, if not rapidly effecting a complete or near-complete clearance, induce tolerance toward tumors and cancers. It’s exactly the same process, and irreversible; as cancers tend to evolve, under extreme pressure, numerous immune evasive features that prevent any recognition of some cells, that timer does not actually begin until the pharmaceutical immune interventions that unmask them are commenced. From the moment those tumors are made visible for an immune response, where they were previously invisible, the clock is ticking toward an IgG4 class switch and a substantial shutdown of the immune response.